Fracture of the trigonal process:
The lateral tubercle on the posterior surface of the talus is also known as the trigonal process. Repeated flexion also predisposes this process to repeated stress, which may result in fracture of this small projection if it gets dislocated. A trigonal process fracture may also result from a sudden injury such as an ankle sprain.
This dislocated fragment produces the same symptoms and is hard to distinguish from an os trigonum. As in normal anatomy, the os trigonum when present is located just behind the trigonal process.
A bony projection on the upper surface of the heel bone (calcaneus) may also lead to crushing of the bony and soft tissue structures during flexion of the foot.
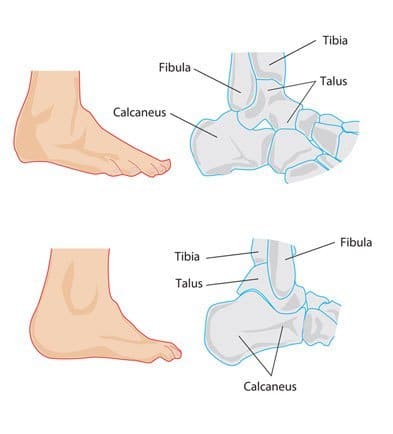
Upper left: Os Trigonum Upper right: Bony prominence on the heel bone (calcaneus)
Lower left: Process of Stieda Lower right: The normal anatomy of ankle
Ankle joint instability resulting from a previous ankle sprain may cause the talus to shift forward during maximum flexion of the foot; as a result, the back of the calcaneus comes in contact with the back of the tibia, crushing the soft tissue structures in between.
Symptoms:
Pain at the back of the ankle during and after activities involving forced downward bending of the foot, such as running down slopes, dancing on toes or kicking
There may be a sharp pain or a dull ache in the region
Tenderness and swelling in the area
Sometimes the pain extends upwards to the calf region or downwards towards the foot.
Diagnosis:
The history of the patient, as well as a thorough clinical examination is important for diagnosing the condition.
Pain can be elicited by turning the foot to the maximum flexed position. A local anesthetic injected at the back of talus eliminates the pain associated with downward flexion of the foot and is a significant diagnostic test for posterior impingement syndrome.
X-rays help to clarify the presence of bony projections, accessory bone or fractured bone fragments in the area.
CT scan and MRI are great diagnostic tools that clearly show the bone and soft tissue condition in the area.
Treatment:
Conservative treatment usually produces significant improvement in the condition and involves giving the sore tissues rest and reducing the pain and inflammation.
The RICE regime is advised and includes:
Rest: Avoiding any activities that cause the pain for about four to six weeks, use of crutches may also be advised
Ice Application: for about 20 minutes at a time, 3-4 times a day for the first two to three days, to reduce swelling and pain in the area .
Compressing the area with the help of elastic bandages; this supports the ankle and prevents inflammation. However, the bandage should not be too tight.
Elevating the leg off the ground above the heart level also reduces inflammation.
Non-steroidal anti-inflammatory painkillers such as ibuprofen, or naproxen may be prescribed.
Steroid (cortisone) injections may be given in the area to reduce inflammation.
If the symptoms are severe, the ankle may be immobilized using a rigid cast or splint.
Ultrasonic and manual massage therapies improve blood flow to the area and speed up healing.
If the condition does not respond well to rest and anti-inflammatory therapy, surgical correction of the cause is required, which entails removing the os trigonum or any bony protuberances and fractured fragments of bone.
Surgery may be performed through an open incision or by using a camera inserted through a small incision. The latter procedure involves fewer complications and a rapid recovery.
In the post-operative healing period, physiotherapy helps to improve strength and control of the ankle as well as increasing the range of motion at the joint.