Things work well when everything is in harmony, arteries take blood in and veins drain the used blood out, maintaining a constant volume of the fascial compartment,
Compartment syndrome starts when the fluid level in the compartment increases. This can occur as a result of:
a severe injury (muscle rupture or bone fracture): blood leaking out from vessels into the tissues => volume increase
infection, toxins (snake bite), excessive exertion: the body defends itself through inflammation, which increases fluid leakage from vessels into the tissues, leading to tissue swelling => volume increase
any physical obstruction to the outflow of blood such as tight bandages, casts, etc., leads to pooling of blood in the compartment => volume increases
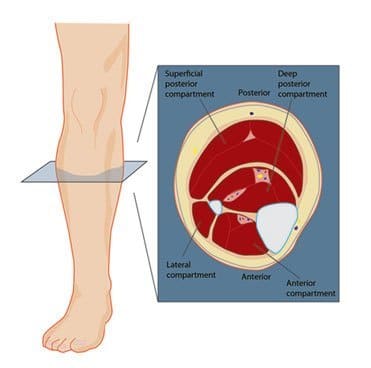
If the volume increases in a compartment, there is no space to expand and the structures within begin compressing. In the anterior and posterior compartments of the leg, there is almost no space to accommodate any extra fluid, and therefore pressure increases rapidly, pressing upon the structures in the compartment, including the blood vessels. When the pressure reaches a significant level, capillaries (the smallest blood vessels) are forced shut. The result is a decreased oxygen supply to the body cells which, in desperate need of oxygen, release chemicals that further increase the leakage of fluid from the vessels, and thus the intra-compartmental pressure rises. This sets off a vicious circle, progressively increasing the pressure to the point where even major blood vessels become compressed, interrupting the blood supply further. If not remedied in time, the lack of blood supply irreversibly damages the muscles, nerves and bones in the compartment and this phenomenon is called “Compartment syndrome”.
Compartment syndrome can be :
Acute, which is usually the result of an injury. There is a rapid increase in intra-compartmental pressure, associated with severe pain. Emergency treatment is needed to prevent permanent damage, or
Chronic (or exertional compartment syndrome) which follows extensive exertion of the muscles in a compartment (as with athletes or marathon runners).
Anterior Compartment Syndrome:
Compartment syndrome most commonly involves the anterior compartment of the leg. The anterior compartment of the lower leg contains four muscles of which the tibialis anterior is the major muscle. This type of injury is quite common in athletes and runners.
Cause:
Anterior compartment syndrome can be either acute or chronic. While the acute syndrome is mainly a result of a direct injury to the muscles in the compartment or fracture of tibia, or an obstruction to the blood flow, chronic compartment syndrome most often results from over-exertion of the muscles or occurs as a sequel to untreated shin splints.
Symptoms:
In acute compartment syndrome:
There is excruciating pain, which is out of proportion to the extent of injury and does not reduce much with the use of painkillers (even morphine) or by elevating the leg.
This severe pain is the result of impairment of nerve function due to lack of oxygen. One may also experience a burning or tightening sensation.
The skin on the front of the leg gets stretched and appears shiny and swollen. Later on, one feels tingling sensations (parasthesia) in the skin.
Pain intensifies on moving the foot or toes (as the muscles in the compartment control these movements).
Bruising may also be present.
In the later stages, paralysis or numbness ensues, which is usually an indication of permanent damage.
Chronic Compartment Syndrome:
This is also known as exertional compartment syndrome, and presents a little differently.
there is dull diffuse pain or muscle cramps
pain increases with activity (due to expansion of blood vessels and increased blood flow in the compartment)
pain subsides after a period of rest
there is numbness in the leg
difficulty in moving foot or toes
there is a visibly swollen or bulging muscle (tibialis anterior) on the anterior side of the leg
Diagnosis:
The symptoms of acute compartment syndrome, especially the exceptionally severe pain, are diagnostic of the condition. One should immediately seek medical attention, even when in doubt.
The diagnosis for both acute and chronic compartment syndrome can be confirmed by measuring the pressure in the compartment.
Treatment:
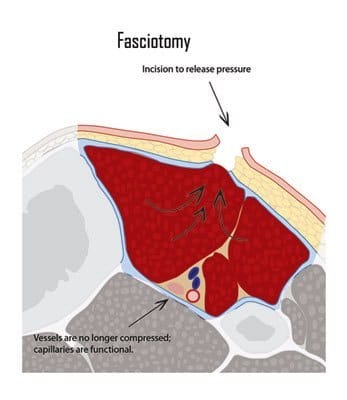
Immediate surgery is the most effective treatment option for acute compartment syndrome. The surgery involves fasciotomy, which is simply cutting open the surrounding unyielding fascia (after incising the skin), to relieve the pressure. In severe cases, the skin is left open for a few days until the swelling subsides. Rarely, a skin graft may be required to bridge the gap.